Real Results
Before & After
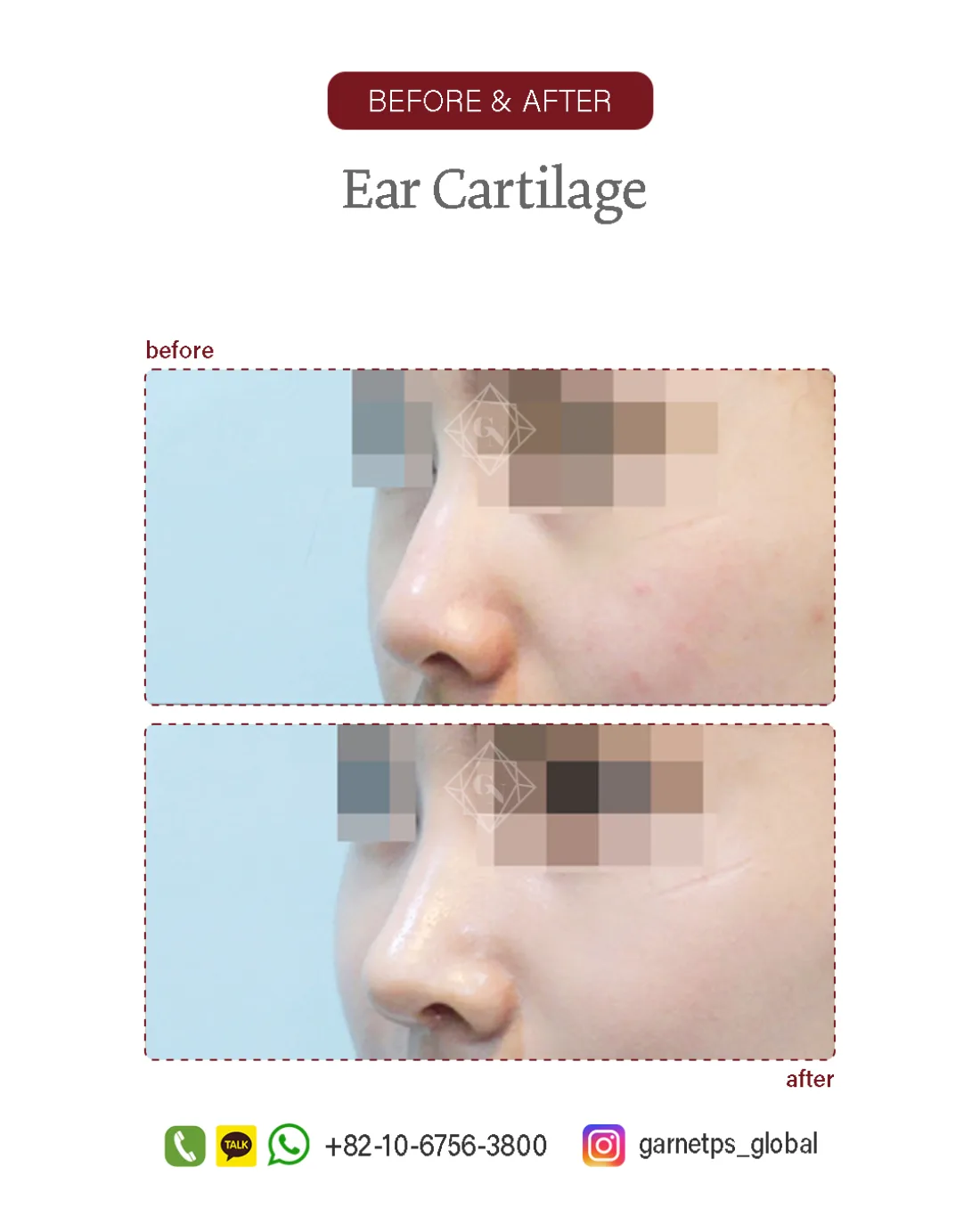
Ear-cartilage rhinoplasty result of an actual Garnet patient, Apgujeong (published with consent; same lighting and angle before and after). Results, recovery and suitability vary by individual and are not guaranteed; further sets are reviewed privately at consultation.

