Real Results
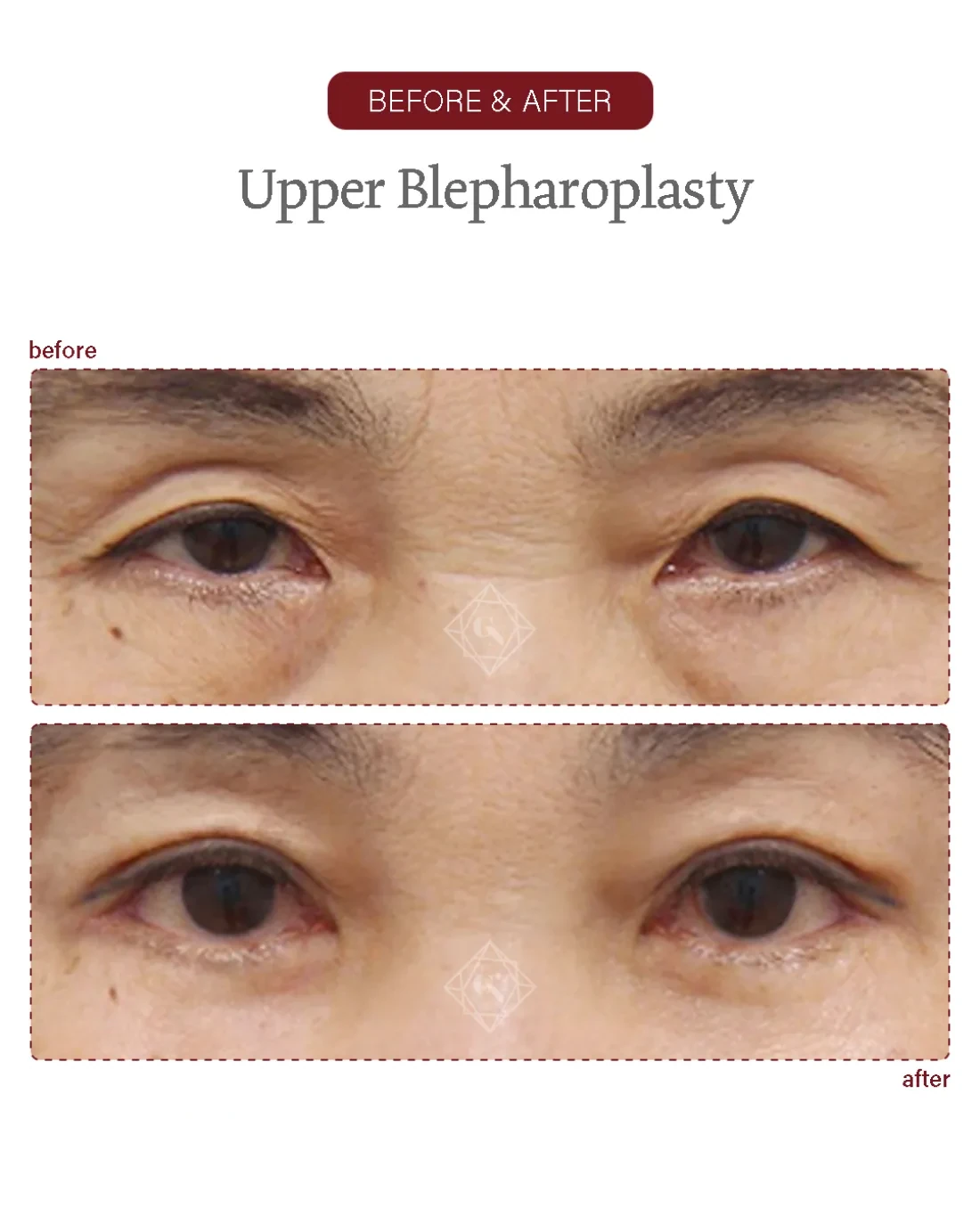
Before & After
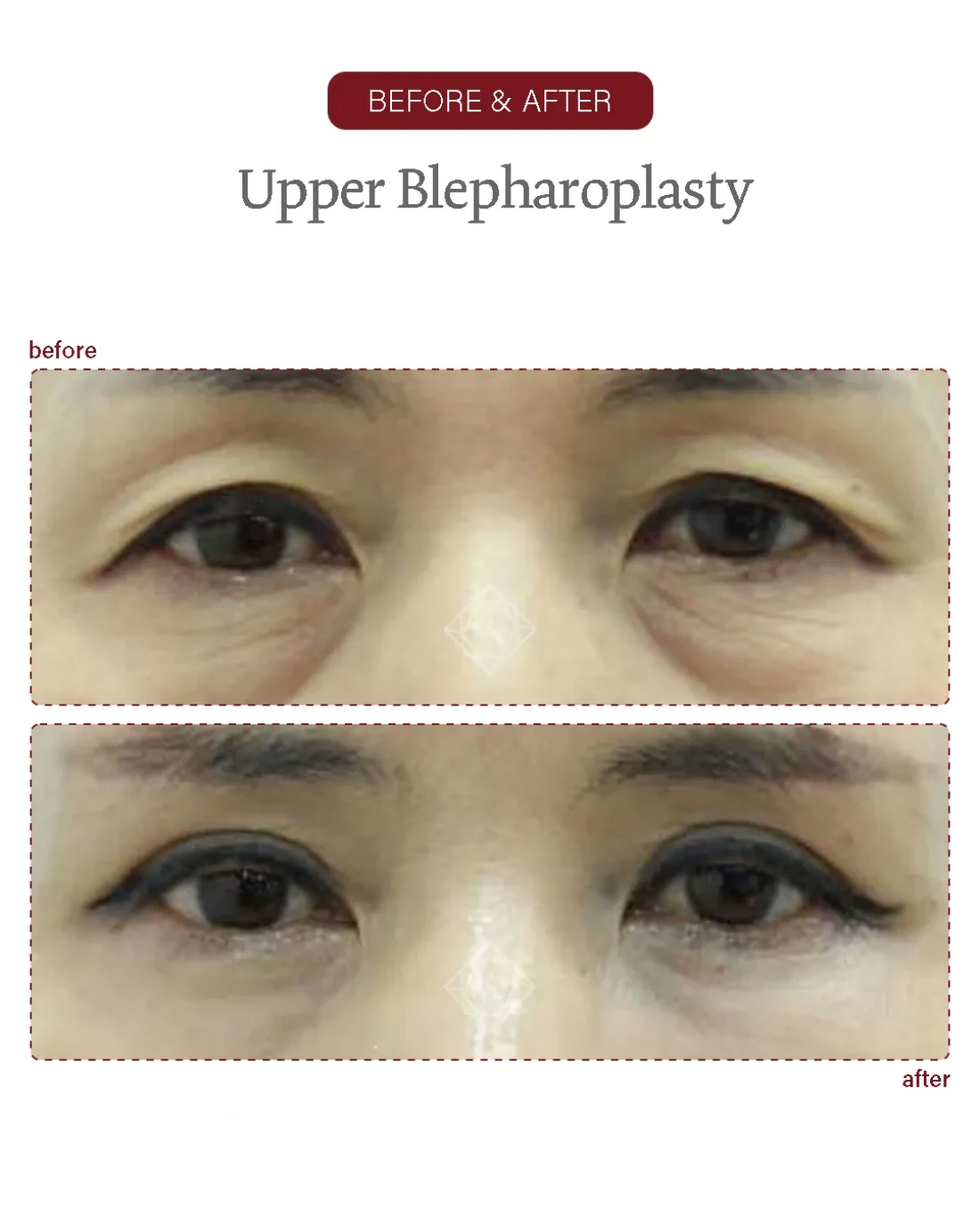
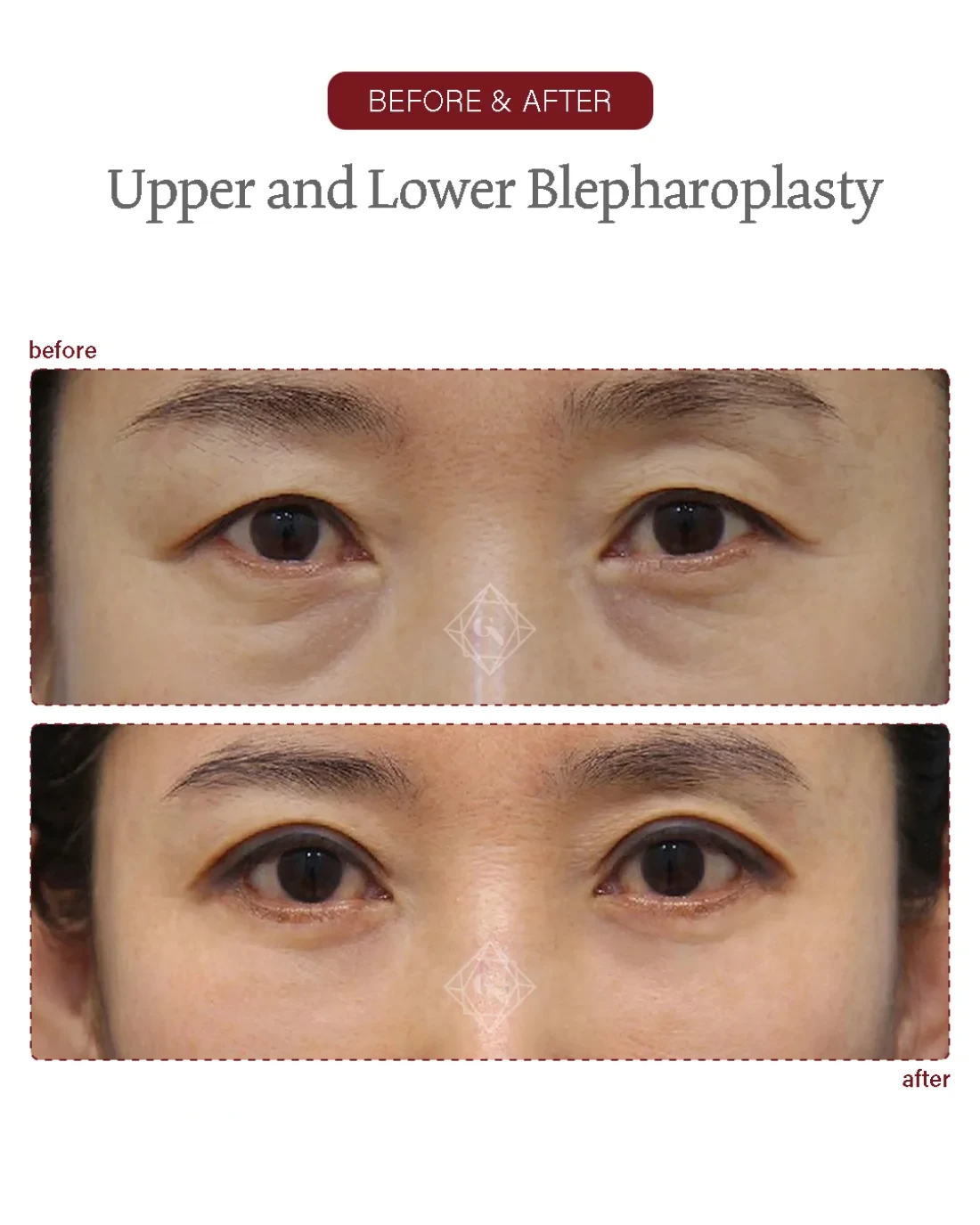
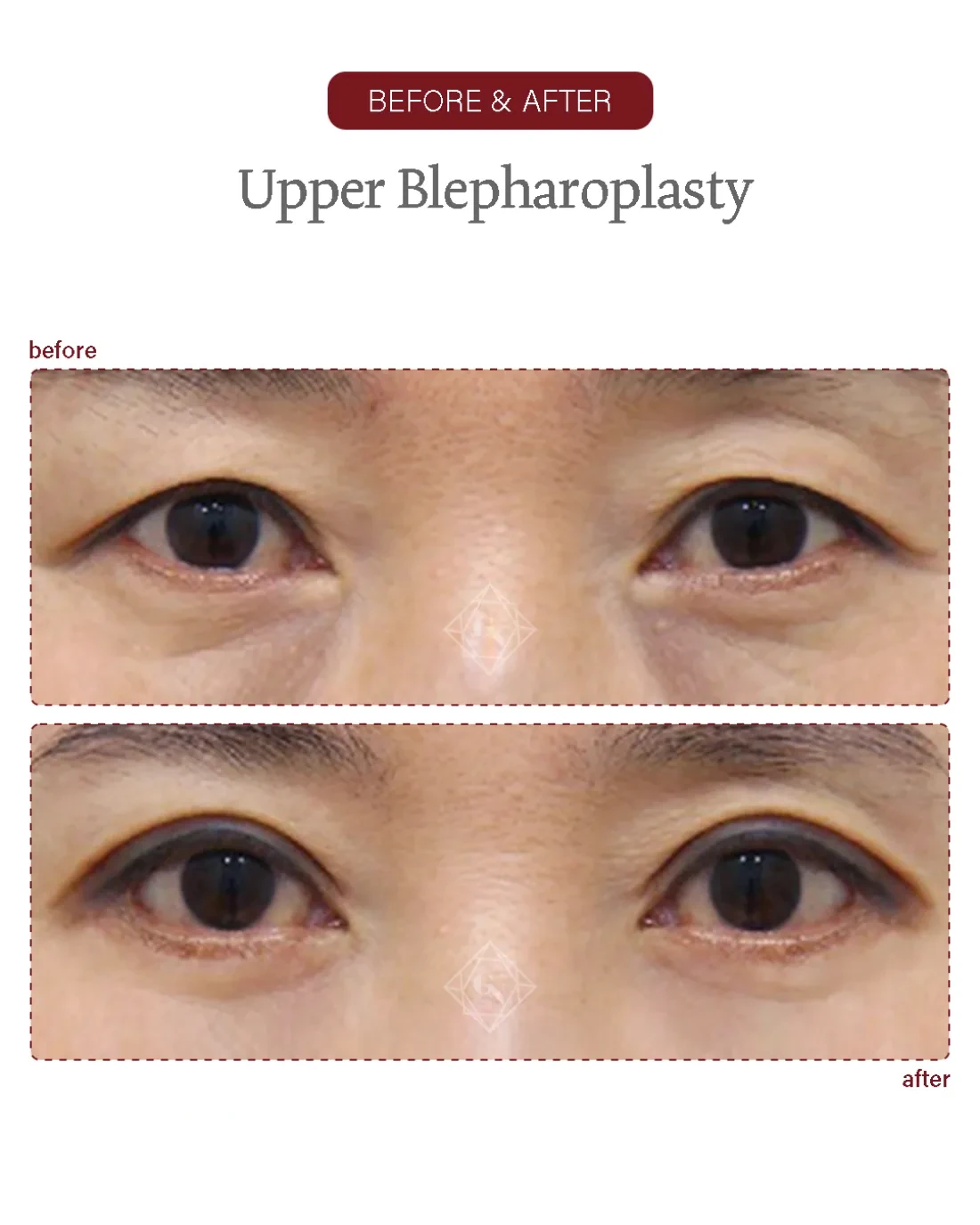
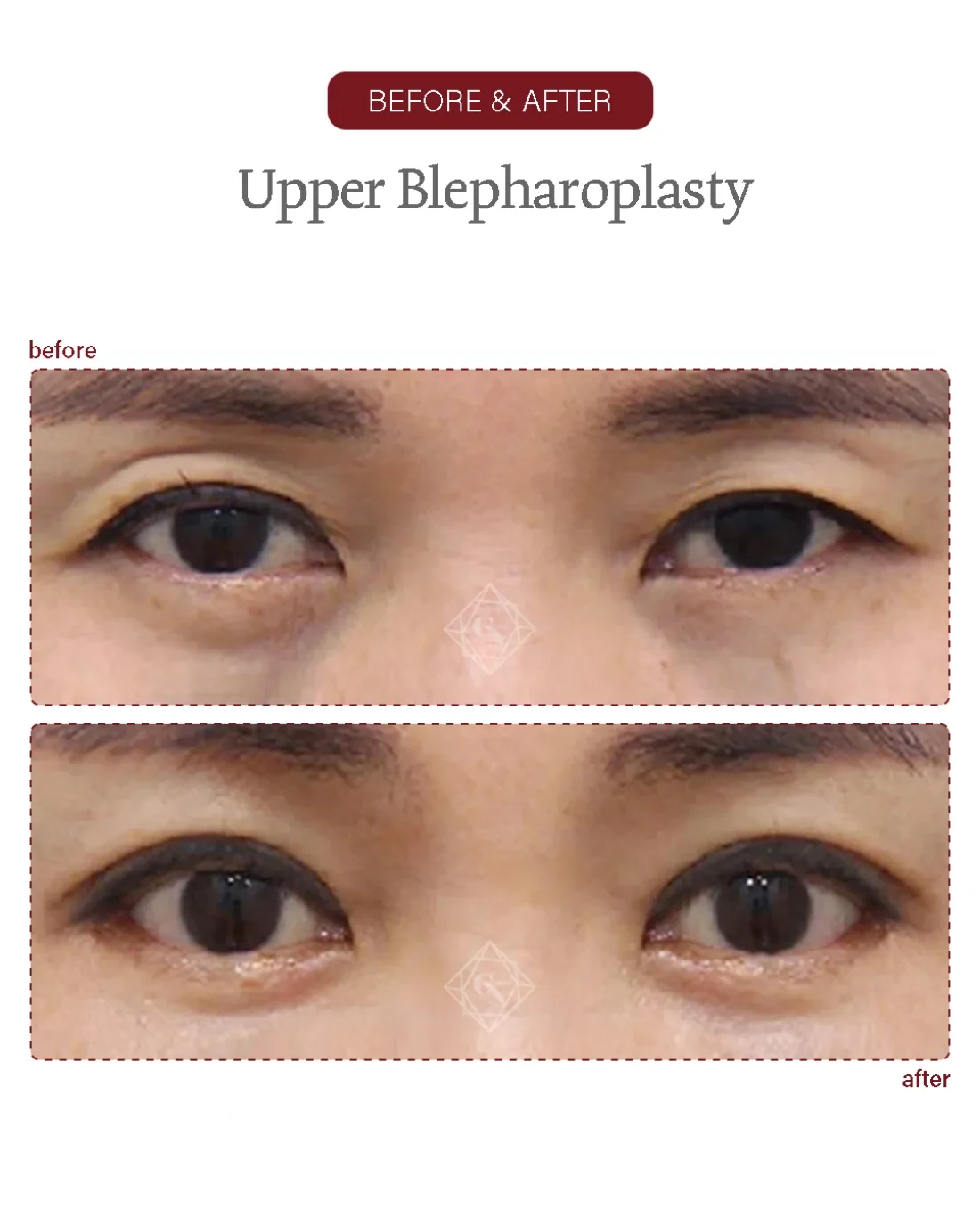
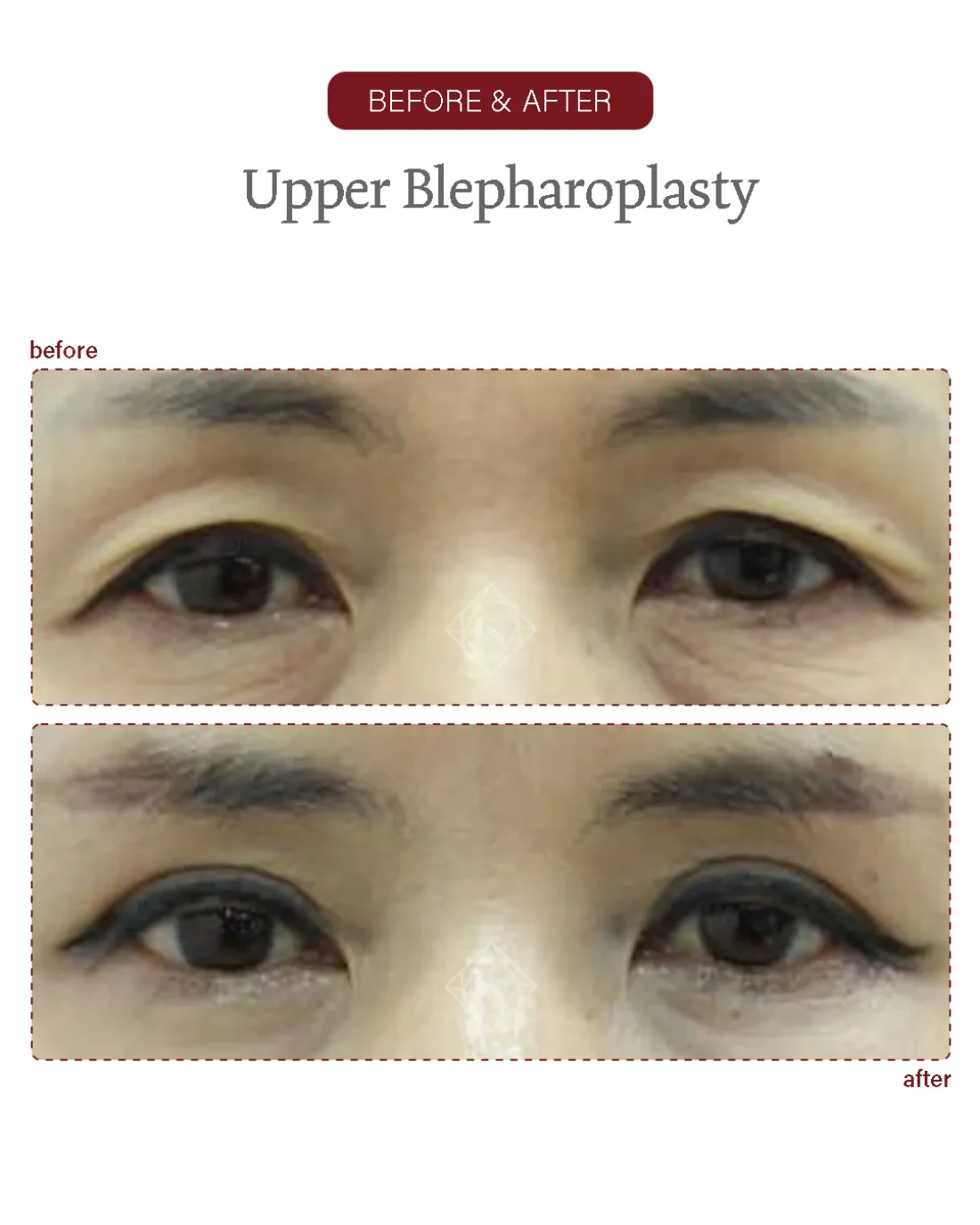
Eyelid before/after examples of actual Garnet patients (published with consent). Results, recovery and suitability vary by individual and are not guaranteed; the right approach is decided at an in-person consultation.
A lower blepharoplasty addresses under-eye bags, the tear-trough hollow and loose lower-lid skin by repositioning fat and re-supporting the eyelid rather than simply removing tissue. At Garnet it is planned and performed by one board-certified plastic surgeon, Dr. In-Soo Baek, from consultation through every follow-up.
Eyelid before/after examples of actual Garnet patients (published with consent). Results, recovery and suitability vary by individual and are not guaranteed; the right approach is decided at an in-person consultation.

Garnet is well known for neck-wrinkle and lifting surgery. The facility is excellent and I’m thoroughly satisfied with the friendly consultation and the surgeon’s skill.
Director Baek In-soo, thank you so much. Thanks to you I keep getting told I look younger — it feels like I’ve gone back to my younger days.
I had upper and lower eyelid surgery and I’m really satisfied. The director and the manager were both so kind and clear.
I started with under-eye fat repositioning — the director and the manager are genuinely kind and good at what they do. I’ll be back.
I came on a referral and was very satisfied thanks to the doctor’s kind consultation and clear explanations. The nurses were friendly too.
I kept reading the reviews and came trusting the many mentions of skill and kindness. The clinic was busy with patients and spotless.
A lower blepharoplasty is an eyelid operation that corrects under-eye bags, the tear-trough hollow and excess lower-lid skin. In the Quad Plus™ four-step approach used at Garnet it repositions herniated orbital fat over the rim, lifts the sub-orbicularis fat (SOOF), suspends the orbicularis muscle and re-drapes the skin — so the hollow is filled and supported rather than the bag simply cut away.
The lower eyelid ages in a few linked ways: the pads of orbital fat behind the eyelid herniate forward and bulge as "bags"; the cheek descends and the ligament between lid and cheek deepens into a tear-trough groove; and the lid skin and orbicularis muscle loosen. Removing fat alone treats only the bulge and can leave the trough — sometimes a deeper hollow — behind.
The Quad Plus™ approach works on all four problems in one operation. Instead of excising the herniated fat, it releases and repositions it across the orbital rim to fill the tear-trough, lifts the SOOF to re-support the mid-face edge, suspends the orbicularis to hold lid position, and re-drapes only the truly redundant skin. The aim is a smooth lid-cheek transition rather than a hollowed, over-resected look.
At Garnet this is a single-surgeon operation. Dr. Baek plans the case from the consultation, performs it himself and reviews healing at set intervals; the clinic caps the day at about two surgeries so each case has unhurried time. The stated aim is to address the concern you arrived with and to prevent foreseeable complications, rather than to chase the maximum possible change.
From the sub-ciliary incision through fat repositioning, the SOOF lift, orbicularis suspension and skin re-draping — every step by Dr. Baek.

A single surgeon, start to finish. Dr. Baek plans the case, performs the operation himself and reviews every follow-up. The clinic caps the day at two surgeries, so each operation has unhurried time.
A lower blepharoplasty at Garnet typically runs about one to two hours, usually under local anaesthesia with sedation as appropriate, decided with you after your medical history is reviewed. The steps below outline how the Quad Plus™ four-step lift is carried out.
Dr. Baek assesses the lid in person — the fat pads, the depth of the tear-trough, skin and orbicularis tone and any lid laxity — and agrees the plan and incision design with you. A snap-back test checks lid support so the right amount of suspension is planned.
A fine transcutaneous (external) incision is placed just below the lash line, where it heals into the natural lid crease. This skin-muscle approach gives access to redrape the skin and is chosen when loose skin needs addressing as well as the fat.
Rather than excising the herniated fat, it is released over the orbital rim and repositioned to fill the tear-trough; the sub-orbicularis oculi fat (SOOF) is lifted to re-support the lid-cheek border, smoothing the groove.
The orbicularis muscle is suspended to add vertical support and hold lid position, which helps reduce the risk of the lid pulling down — a key step where any laxity is present.
Only the truly redundant skin is conservatively trimmed and re-draped without tension. Where the consultation shows it, upper eyelid surgery or ptosis correction may be combined in the same sitting.
Fine closure and a light dressing. Because Garnet is single-surgeon, Dr. Baek reviews you himself before you settle in and at each follow-up; sutures come out at about seven days.

The trademarked Quad Plus™ describes Garnet's named four-step lower-blepharoplasty technique — fat repositioning, SOOF lift, orbicularis suspension and skin re-draping. Trademark registration describes the named technique, not a superior outcome.
Three structures explain the ageing lower lid: the orbital fat pads (medial, central and lateral), held back by the orbital septum; the arcus marginalis and the orbicularis-retaining ligament, which tether the lid to the bony rim and create the tear-trough as the face descends; and the orbicularis oculi muscle and lid skin, which lose tone. Releasing the arcus marginalis lets herniated fat be redraped across the rim to soften the groove rather than excised (Momosawa et al., Aesthetic Surg J 2008; DOI 10.1016/j.asj.2008.02.002).
Because the trough is caused by tethering and volume loss — not only by the bag — supporting the lid and repositioning fat addresses the cause directly, which is what helps the result sit smoothly. Where lid laxity is present, suspending the orbicularis adds vertical support and is associated with a safer lid position after surgery (J Craniofac Surg 2024; DOI 10.1097/SCS.0000000000009716). Garnet plans the release and the amount of skin to re-drape individually for each face; for younger patients whose main issue is the bag and trough alone, under-eye fat repositioning through a hidden inner-lid route may be more proportionate.
| Fat removal only | Quad Plus™ lower blepharoplasty | Under-eye fat repositioning | |
|---|---|---|---|
| Main concern | Under-eye bag | Bag + tear-trough + loose skin | Bag + tear-trough, skin good |
| Fat handled by | Excised | Repositioned over the rim | Repositioned (inner-lid route) |
| Loose skin treated | No | Yes — skin re-draped | No |
| Scar | Varies | Hidden sub-ciliary line | No external scar (inner lid) |
| Typical candidate | Limited use now | Older lid, skin laxity | Younger lid, good skin |
Repositioning rather than removing fat is associated with a smoother lid-cheek transition and low recurrence in published transcutaneous series (Saudi J Ophthalmol 2025; DOI 10.4103/sjopt.sjopt_89_25). The right choice is individual — a younger patient with good skin may suit under-eye fat repositioning instead; Dr. Baek advises at consultation.
A lower blepharoplasty is usually performed under local anaesthesia with light sedation, decided with you for comfort over a one-to-two-hour operation. Your medical history and any dry-eye tendency are reviewed beforehand.
Because Garnet caps the day at about two surgeries, the operation is unhurried and the same surgeon who planned the case carries it out and reviews recovery — there is no separate operating doctor and no rotation of care.
Garnet is registered with Korea's foreign-patient programme; pre-operative checks, scheduling and after-care are coordinated for international visitors in English.
If surgery is not appropriate, or a lighter inner-lid option suits you better, that is said at the consultation. Photos can be reviewed before you travel.
The Quad Plus™ lower blepharoplasty uses a transcutaneous (external) incision placed just beneath the lash line, so the scar settles into the natural lower-lid crease. Closed without tension and following an existing contour, it is usually fine and not obvious in everyday settings once mature. Where loose skin is the issue, this external route is preferred because it allows the skin to be re-draped.
Scars are permanent but designed to hide along the lash line; healing varies by individual and skin type. By contrast, a younger patient whose skin is good and whose concern is the bag and trough alone may be suited to an inner-lid route with no external scar — discussed at consultation. Dr. Baek reviews scar maturation at the 1-, 3- and 6-month visits and advises on scar care.
Keep the head elevated, use cold compresses early, take medication and any eye drops as prescribed, sleep on your back, and keep your follow-up visits.
Rubbing the eyes, strenuous exercise and heavy lifting early on, alcohol and smoking, very hot showers/saunas, eye make-up until cleared, and direct sun on healing scars.
A lower blepharoplasty does not stop the eye area ageing, but repositioning fat rather than removing it is intended to give a durable, natural under-eye contour because the volume that fills the trough stays in place. Published transcutaneous series with conservative skin resection and orbicularis support report lasting correction with low recurrence and revision rates (Saudi J Ophthalmol 2025; DOI 10.4103/sjopt.sjopt_89_25).
Individual longevity depends on tissue quality, sun exposure, skin care and how the face ages afterwards. Skin-surface ageing — fine lines and pigment — continues independently and can be maintained separately over time. Garnet's approach is to support the lid and reposition volume so the result sits smoothly from the start, since an under-eye that was never over-resected tends to age more gracefully.
Many patients plan upper blepharoplasty in the same sitting, since the upper and lower lids age together and a balanced result looks more rested than tighter.
Where the upper lid also sits low, ptosis correction can open the eye while the lower lid is refined, for an even, alert look.
An incision or non-incision double-eyelid may be combined where crease definition is part of the concern.
Fat grafting can restore lost volume in the cheek or temple that under-eye work alone does not replace, for overall balance.
Every operation carries risk. For lower blepharoplasty the most discussed concern is a change in lid position — scleral show (the white showing below the iris) or, uncommonly, ectropion (the lid pulling away) — which is why suspending the orbicularis and conservative skin removal matter; in refined transcutaneous series with these steps, increased scleral show occurred in about 1% and most settled (Saudi J Ophthalmol 2025; DOI 10.4103/sjopt.sjopt_89_25).
Other possible risks include temporary swelling and bruising, asymmetry, dryness or watering, sensitivity, scar-related issues and, rarely, the need for a touch-up. Pre-existing dry eye or marked lid laxity raises some of these and is assessed beforehand. These are explained individually at consultation.
What reduces risk in practice: careful patient selection and lid-laxity assessment, repositioning rather than over-removing fat, conservative skin resection, orbicularis support and follow-up by the operating surgeon. Garnet's single-surgeon, low-volume model is built around exactly this kind of unhurried planning and personal after-care. Results are intended improvements, not guarantees.
Most international patients plan roughly 7–10 days in Korea for a lower blepharoplasty, so sutures can be removed by the surgeon at about day seven and the early swelling has settled before travel. The coordinator confirms the timing for your specific plan.
Before you travel, send clear photos (front, looking up, and a relaxed three-quarter view) and a note on your concern and dates through WhatsApp, LINE or the form below. You'll get an honest pre-assessment — including whether surgery or a lighter inner-lid option fits — rather than a hard sell.
Garnet is registered with Korea's foreign-patient programme and coordinates consultations, scheduling and after-care in English. After you return home, Dr. Baek can continue to review your recovery by messenger.
| Fat removal only | Quad Plus™ lower blepharoplasty | Under-eye fat repositioning | |
|---|---|---|---|
| Main concern | Under-eye bag | Bag + tear-trough + loose skin | Bag + tear-trough, skin good |
| Fat handled by | Excised | Repositioned over the rim | Repositioned (inner-lid route) |
| Loose skin treated | No | Yes — skin re-draped | No |
| Scar | Varies | Hidden sub-ciliary line | No external scar (inner lid) |
| Typical candidate | Limited use now | Older lid, skin laxity | Younger lid, good skin |
Citations are provided for general education. This page is informational and does not replace an in-person consultation; suitability, technique and recovery are individual.
Send photos and your question before you travel. An English-speaking coordinator reviews every enquiry and replies with honest guidance on whether surgery is appropriate, the likely plan and timing.
Prefer to chat now? Reach the coordinator directly: