A single surgeon, start to finish. Dr. Baek plans the case, performs the operation himself and reviews every follow-up. The clinic caps the day at two surgeries, so each operation has unhurried time.
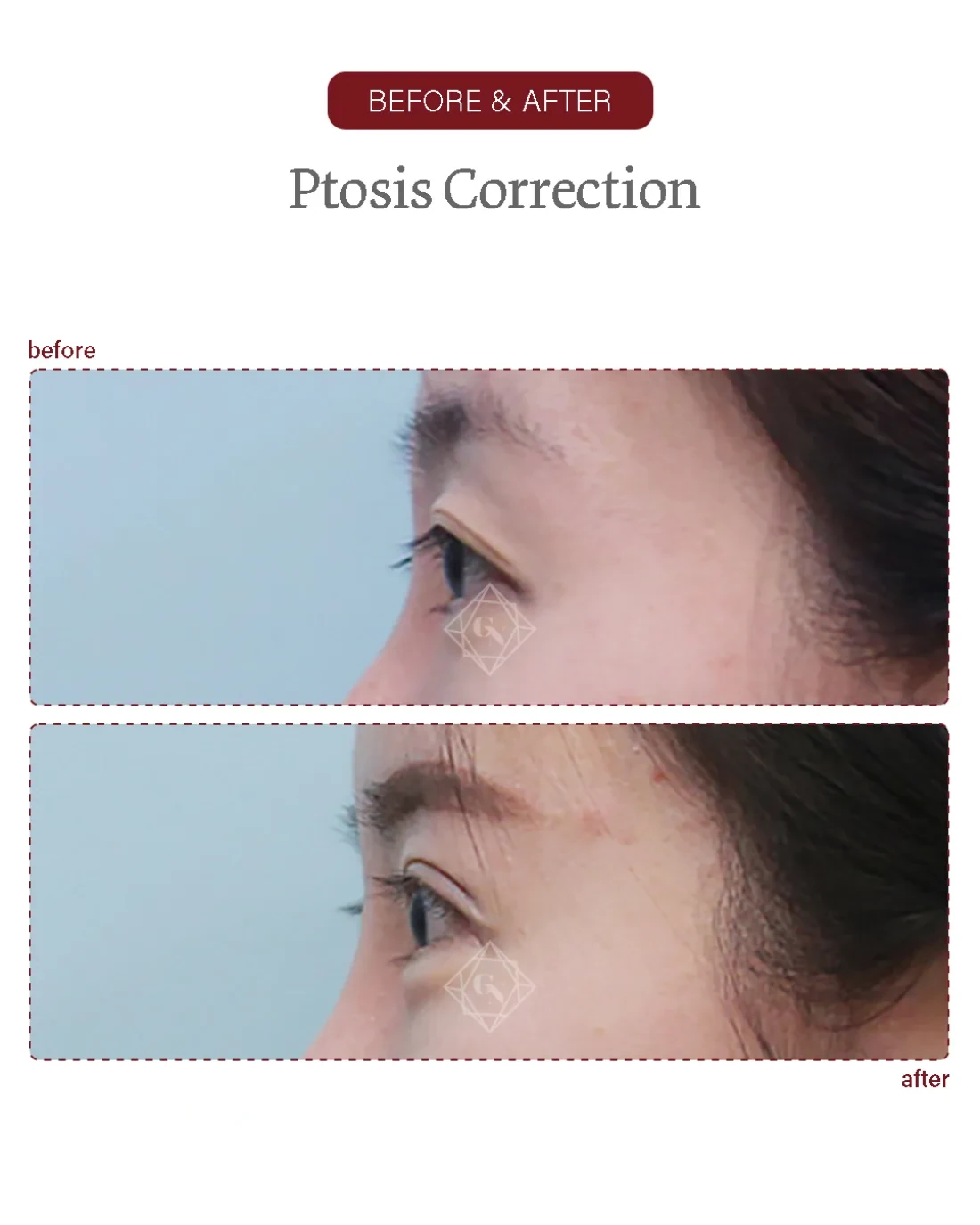
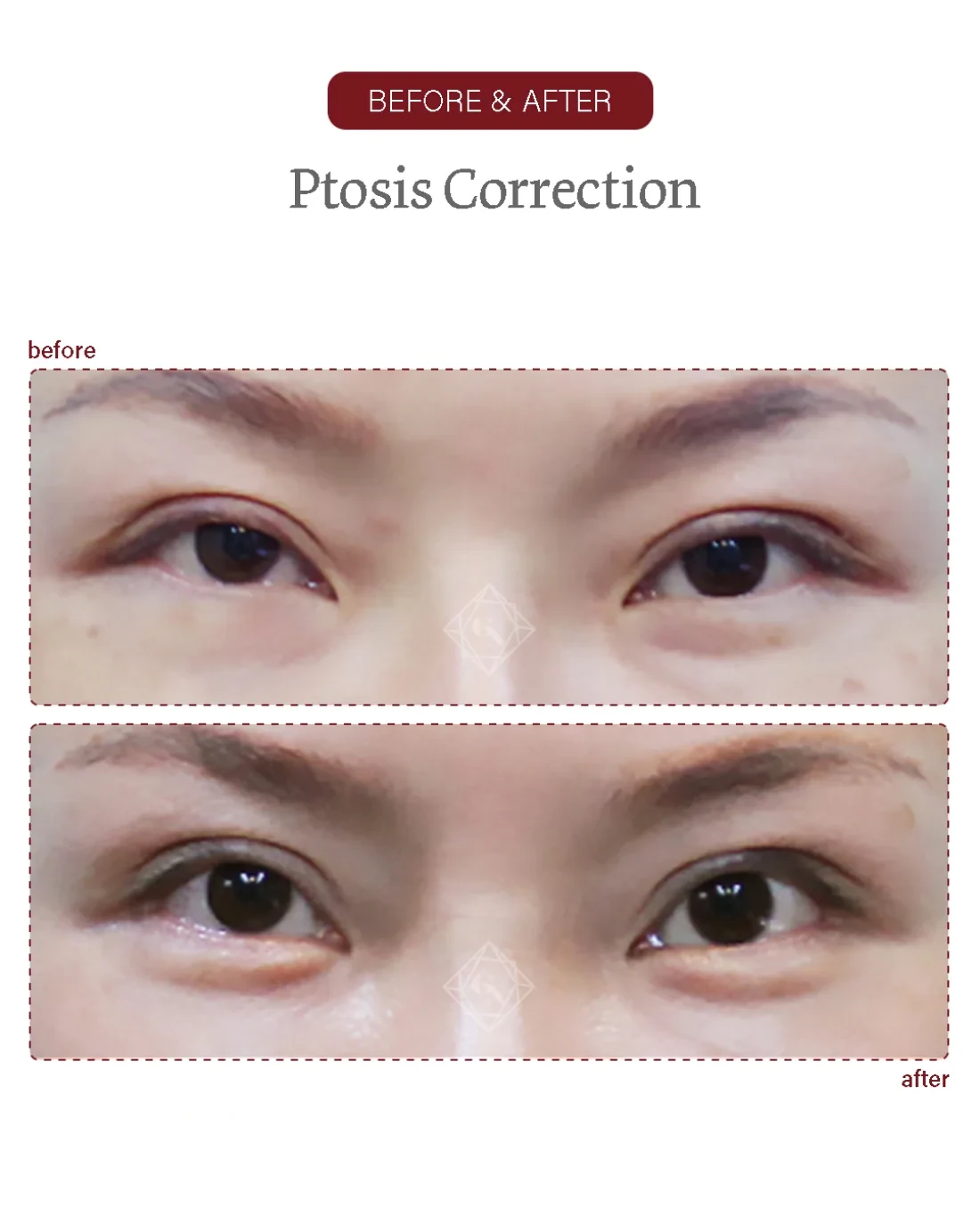
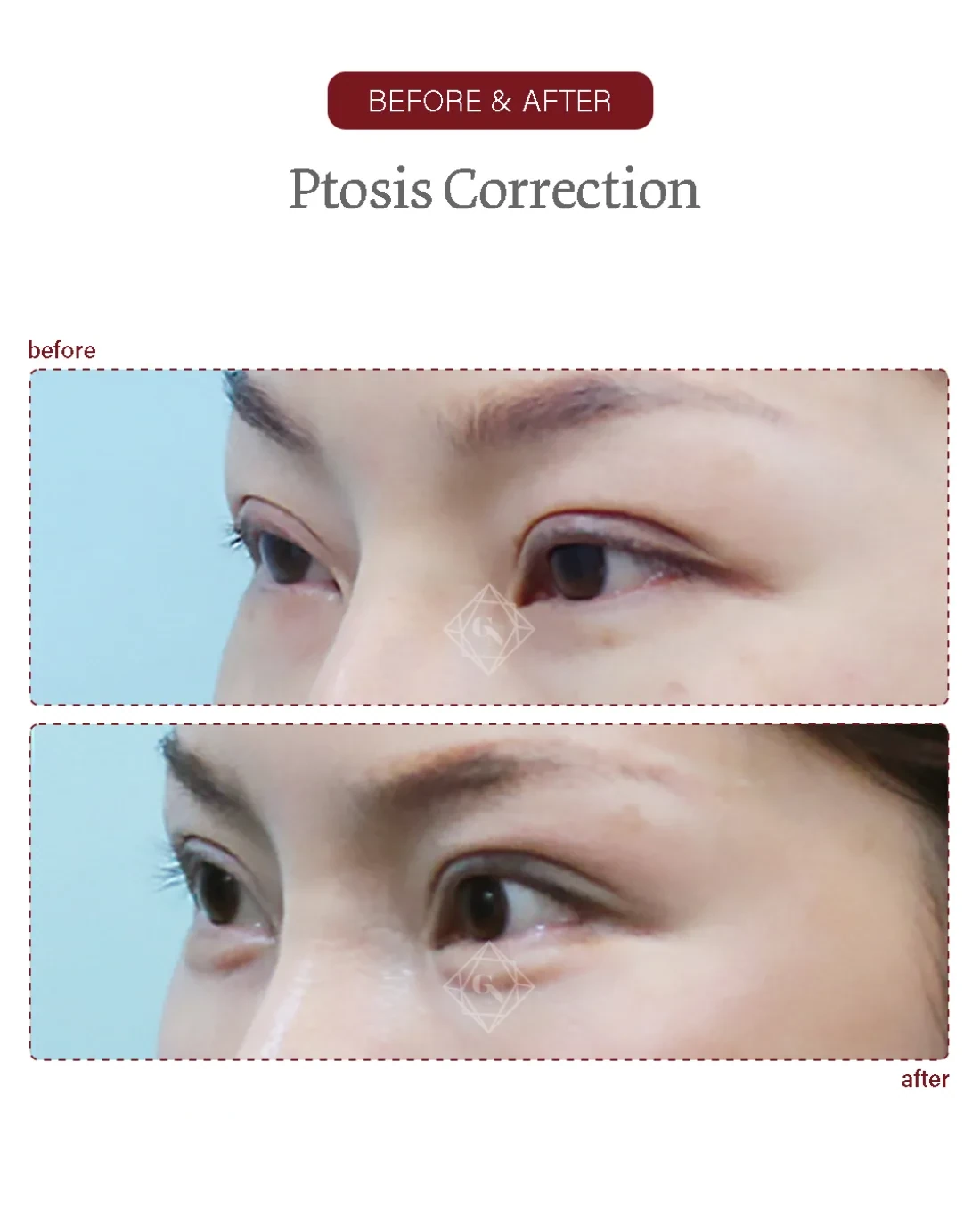
Ptosis correction at Garnet typically runs about one to one-and-a-half hours, usually under local anaesthesia with sedation as appropriate, decided with you after your medical history is reviewed; light anaesthesia lets you cooperate so lid height can be checked during surgery. The steps below outline how it is carried out.