Real Results
Before & After
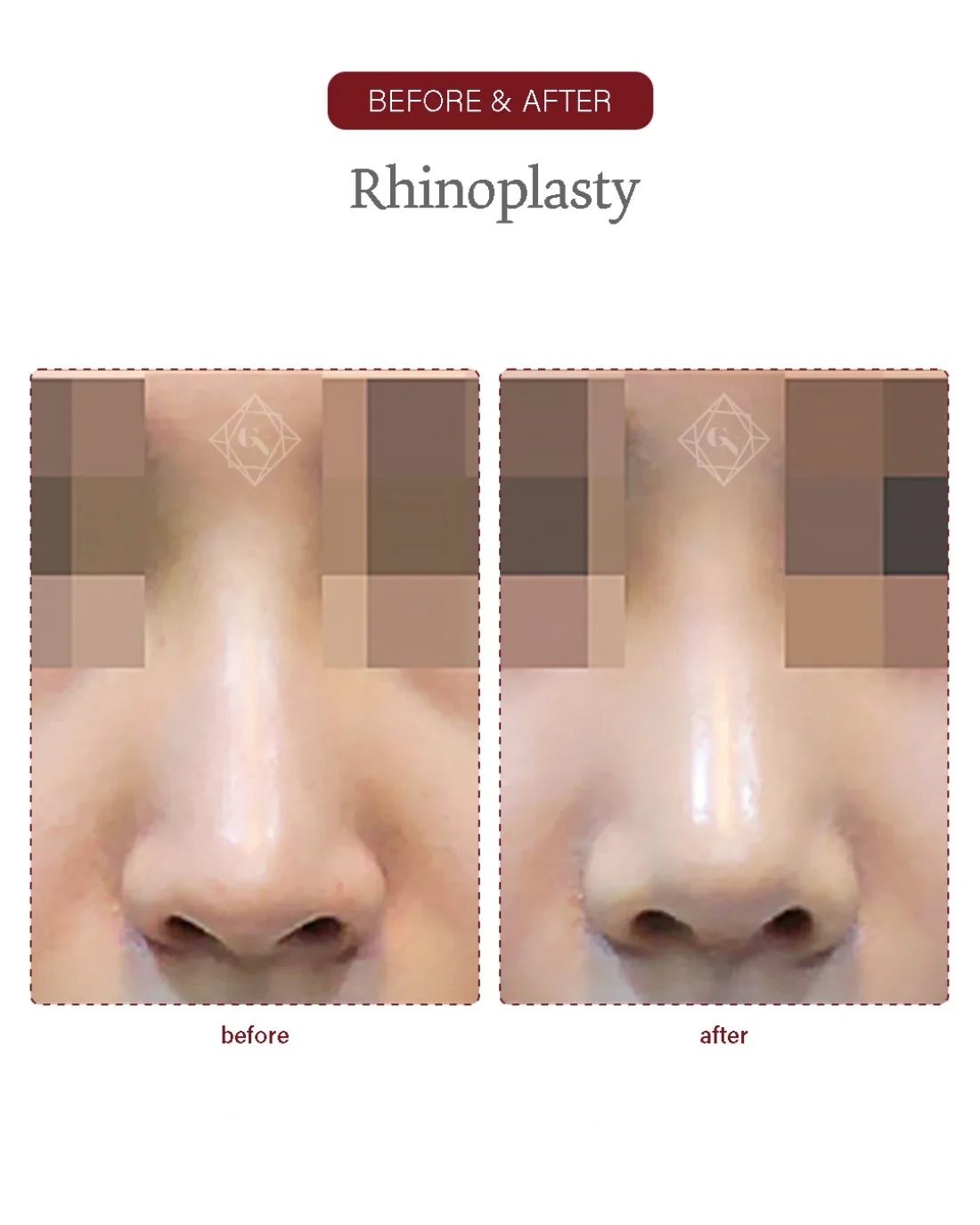
Rhinoplasty result of an actual Garnet patient (published with consent). Date, procedure and clinic (Garnet Plastic Surgery, Apgujeong) are labelled on the image, with the usual same-condition disclaimer. Results, recovery and suitability vary by individual and are not guaranteed.

