Real Results
Before & After
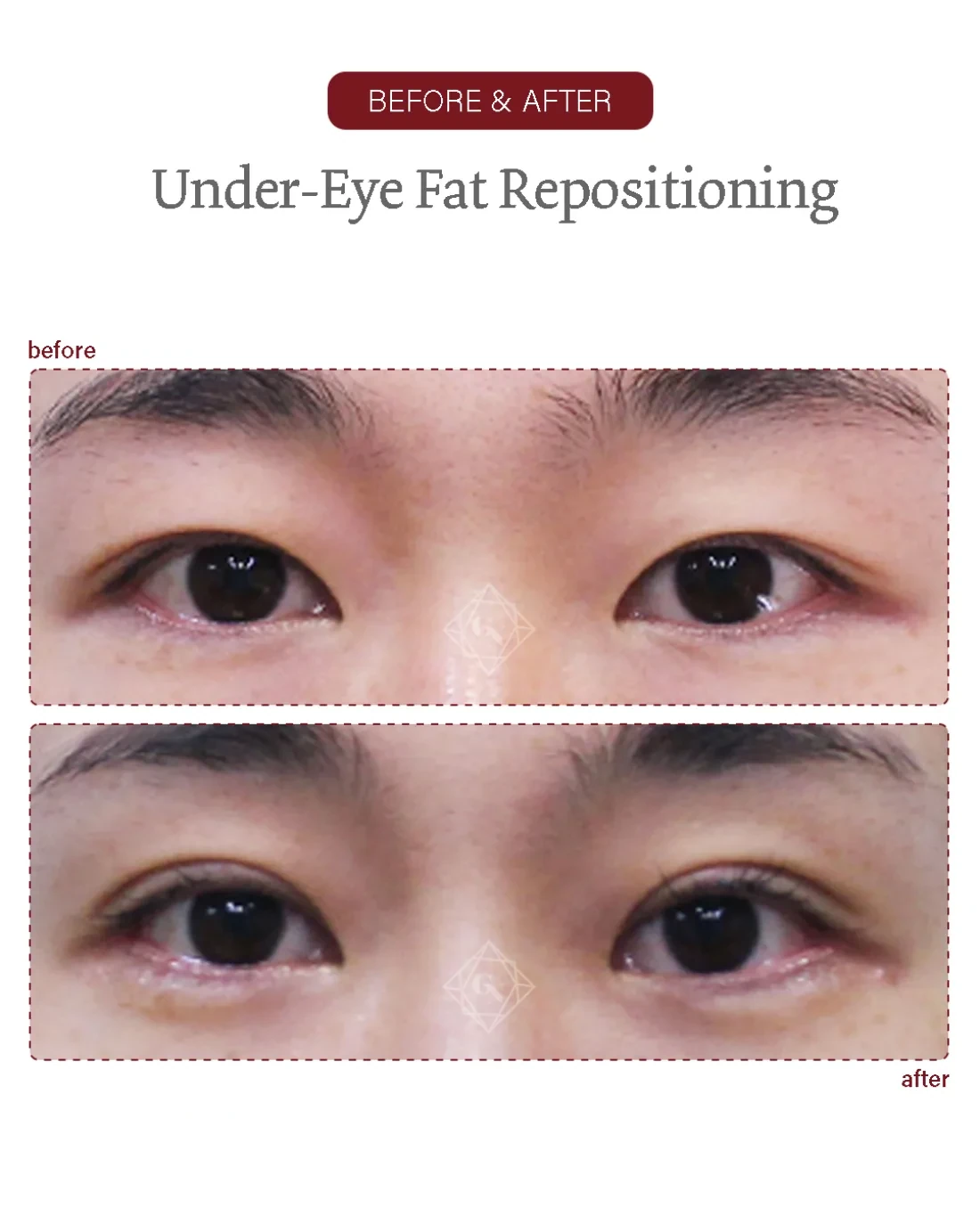
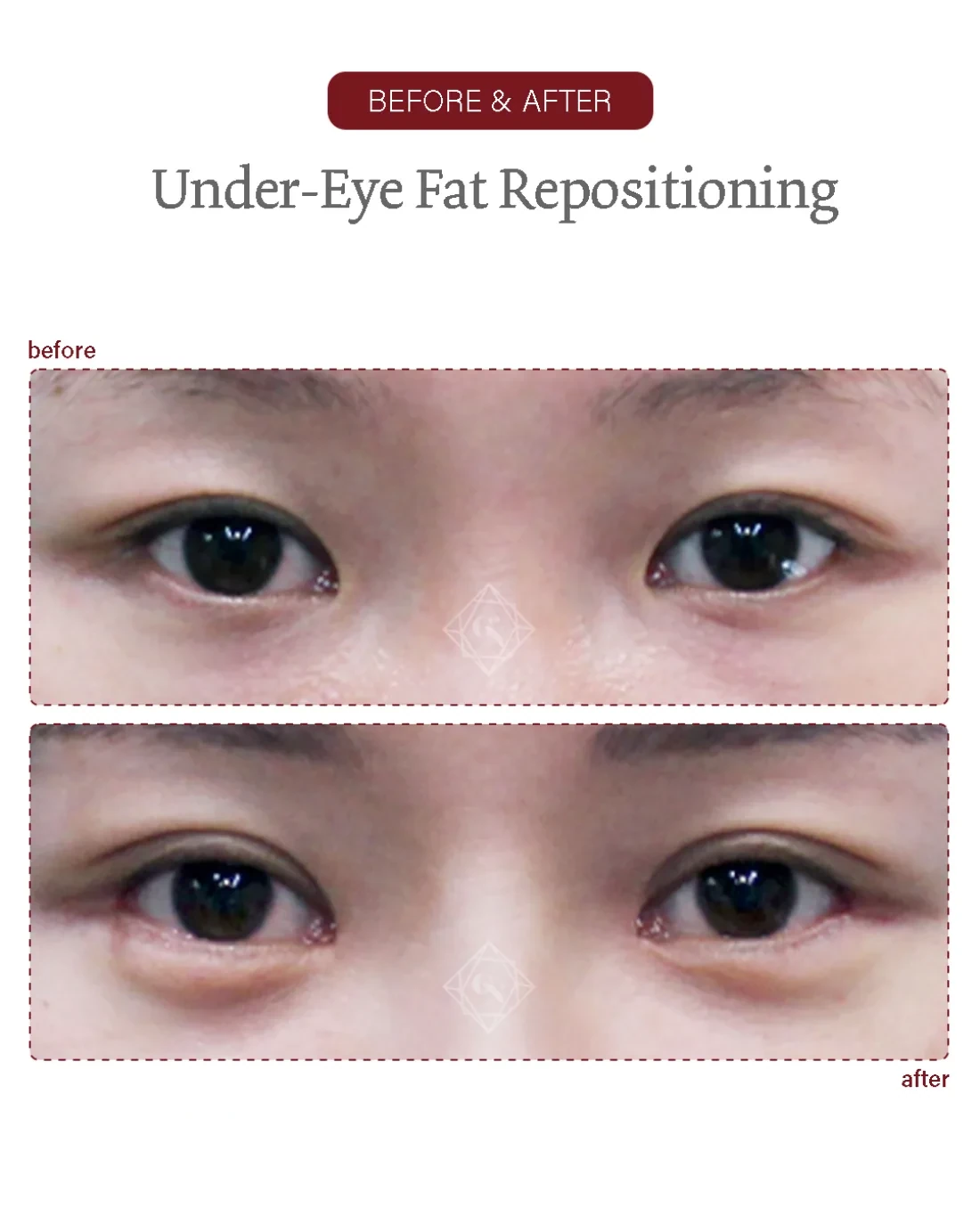
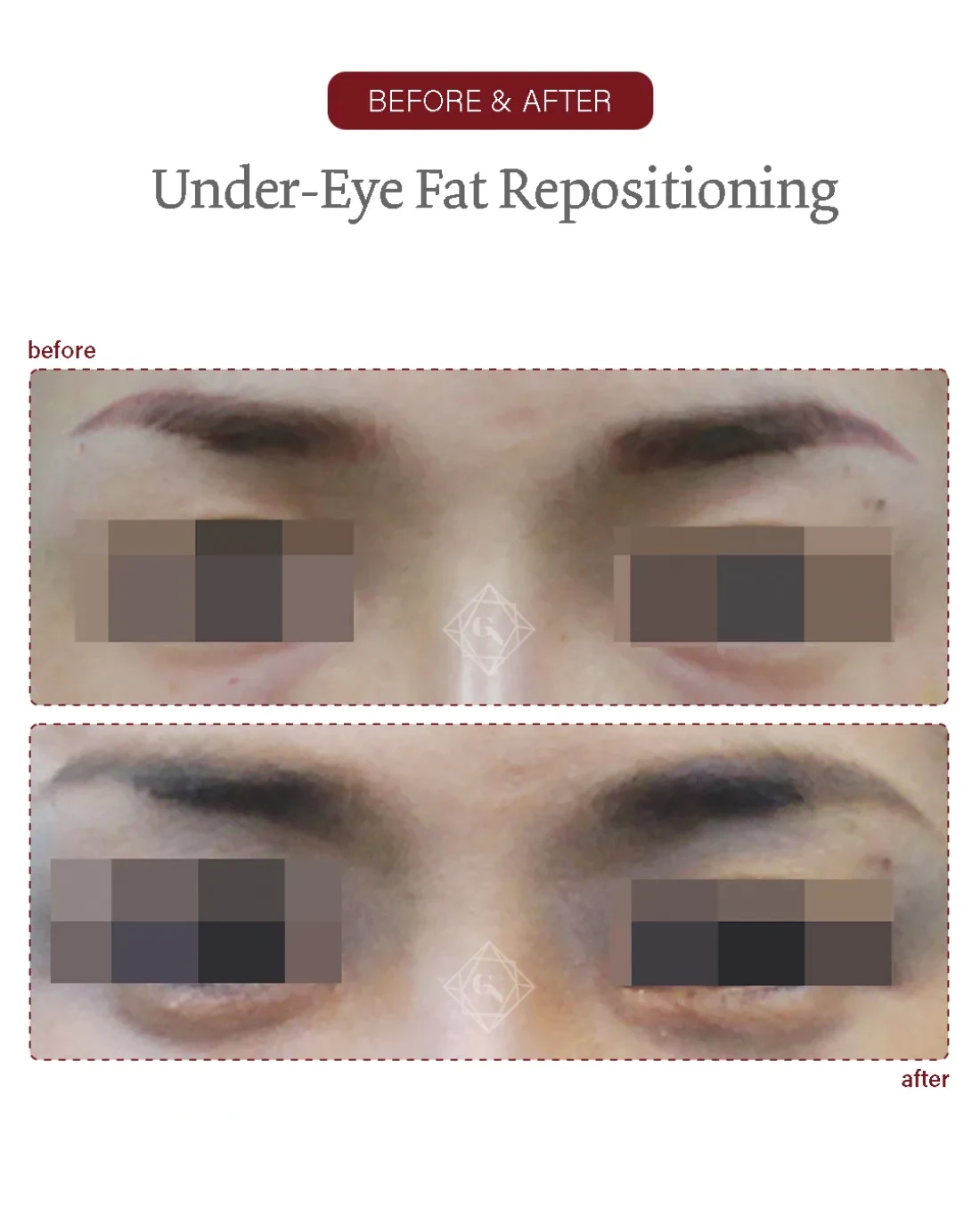
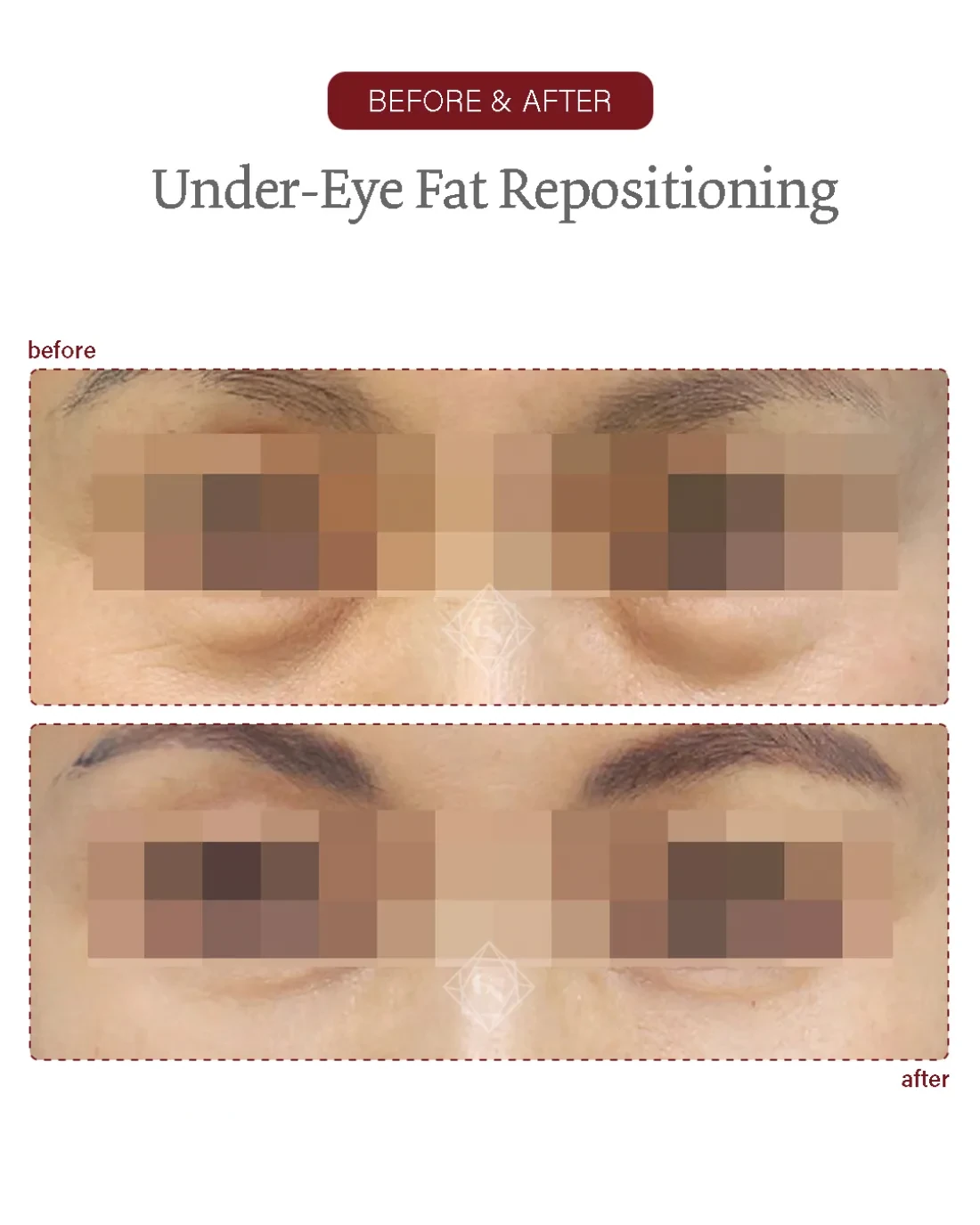
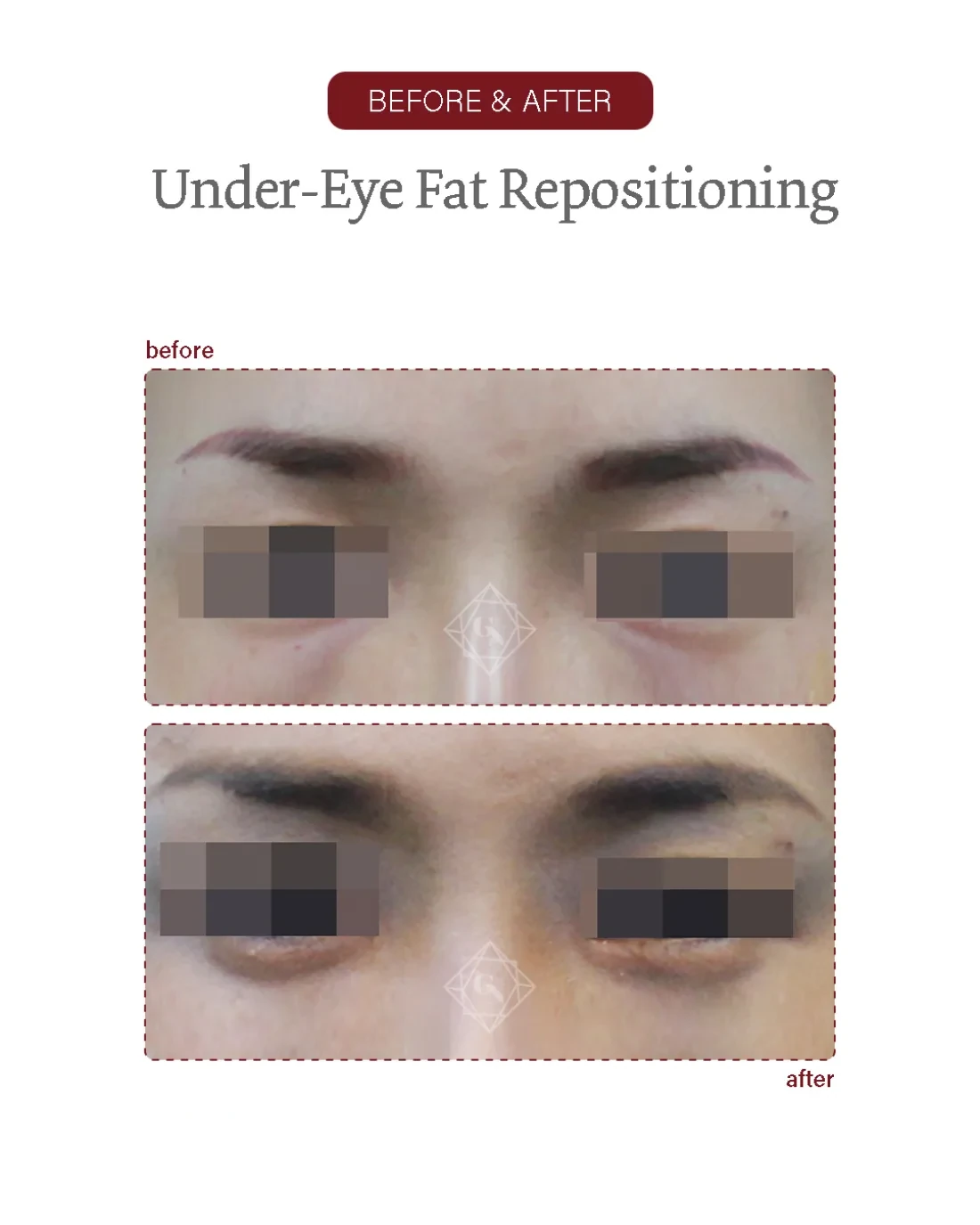
Under-eye fat repositioning before/after of actual Garnet patients (published with consent; each set labelled with date, procedure and clinic). Photographed under comparable conditions. Results, recovery and suitability vary by individual and are not guaranteed.

