Real Results
Before & After
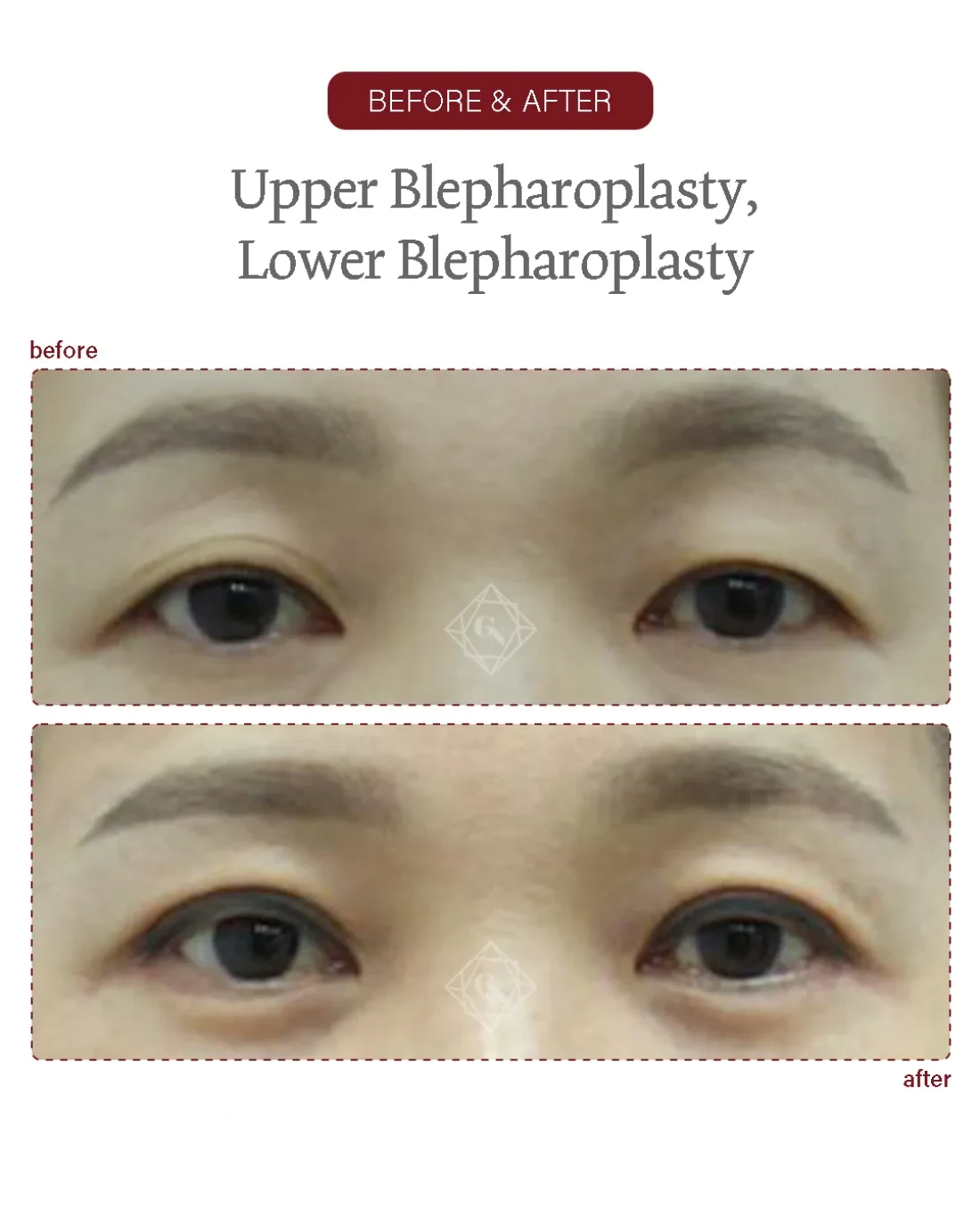
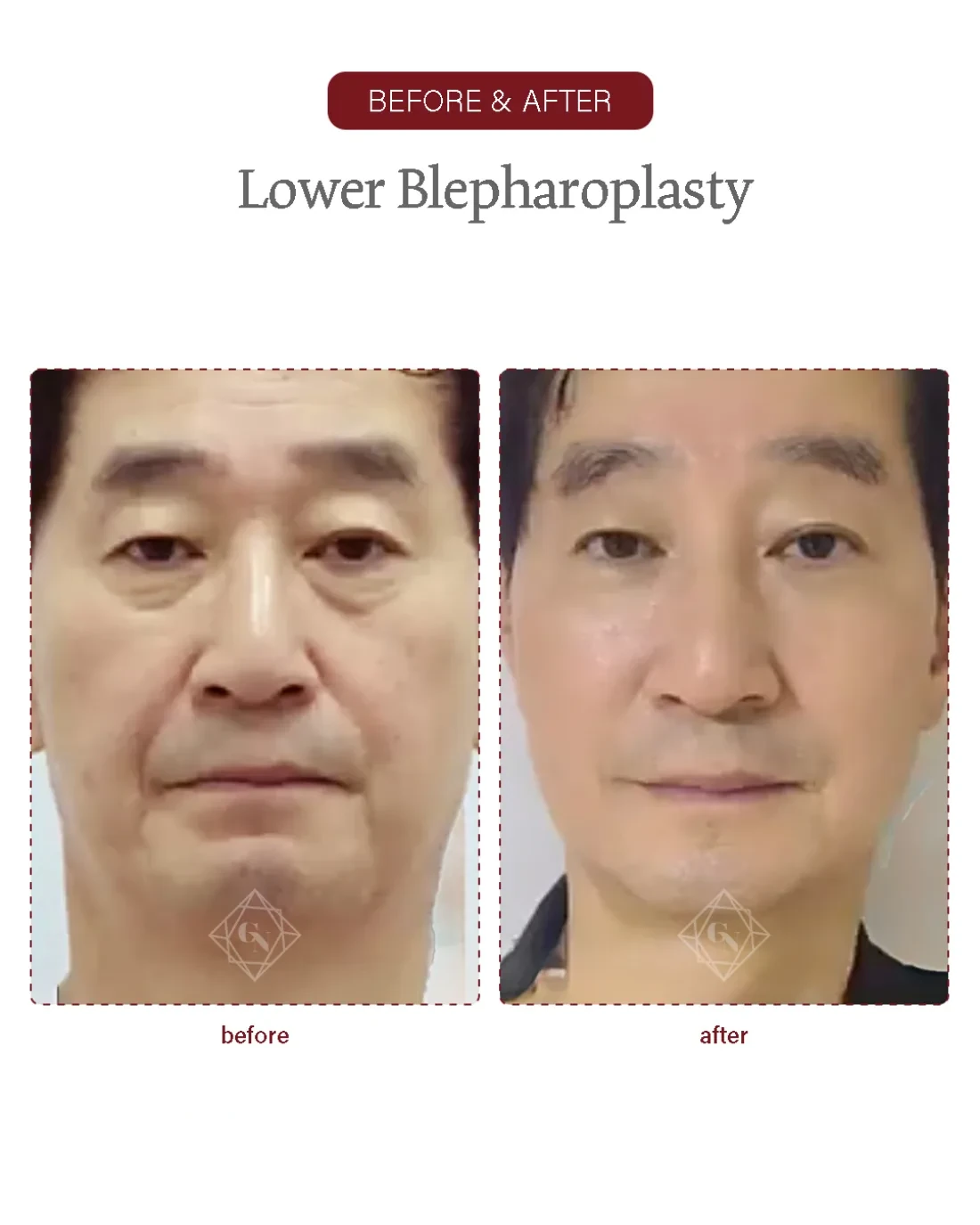
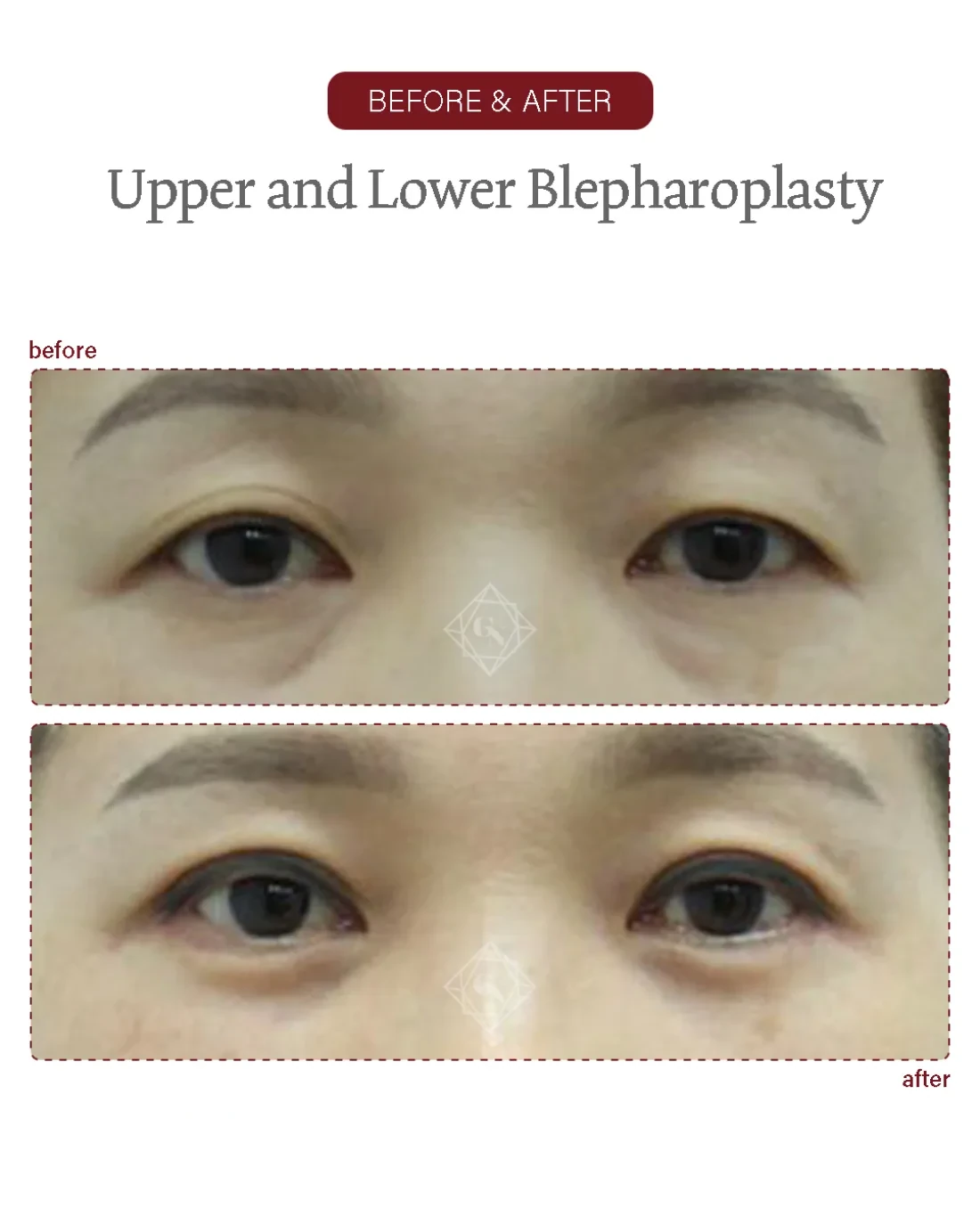
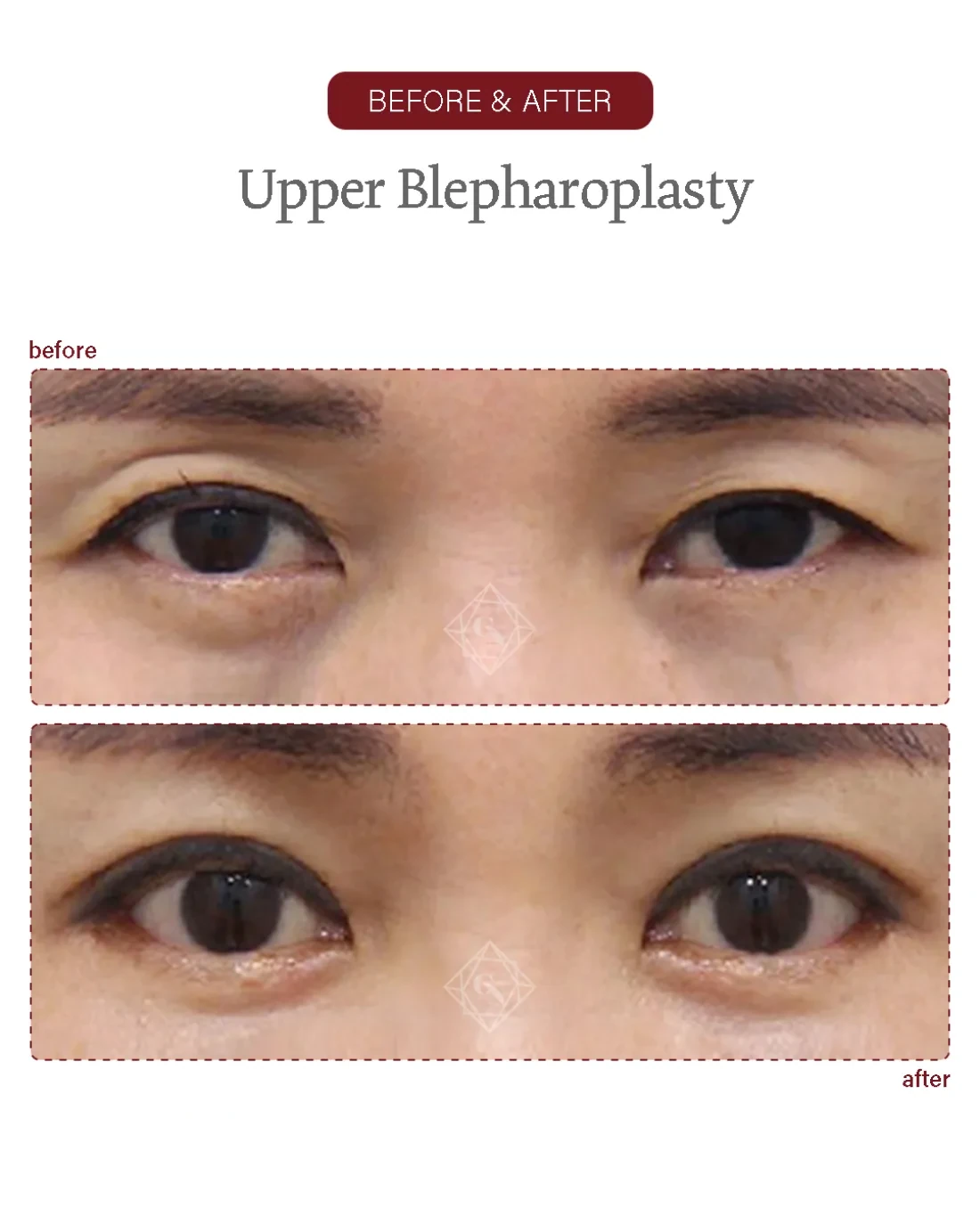
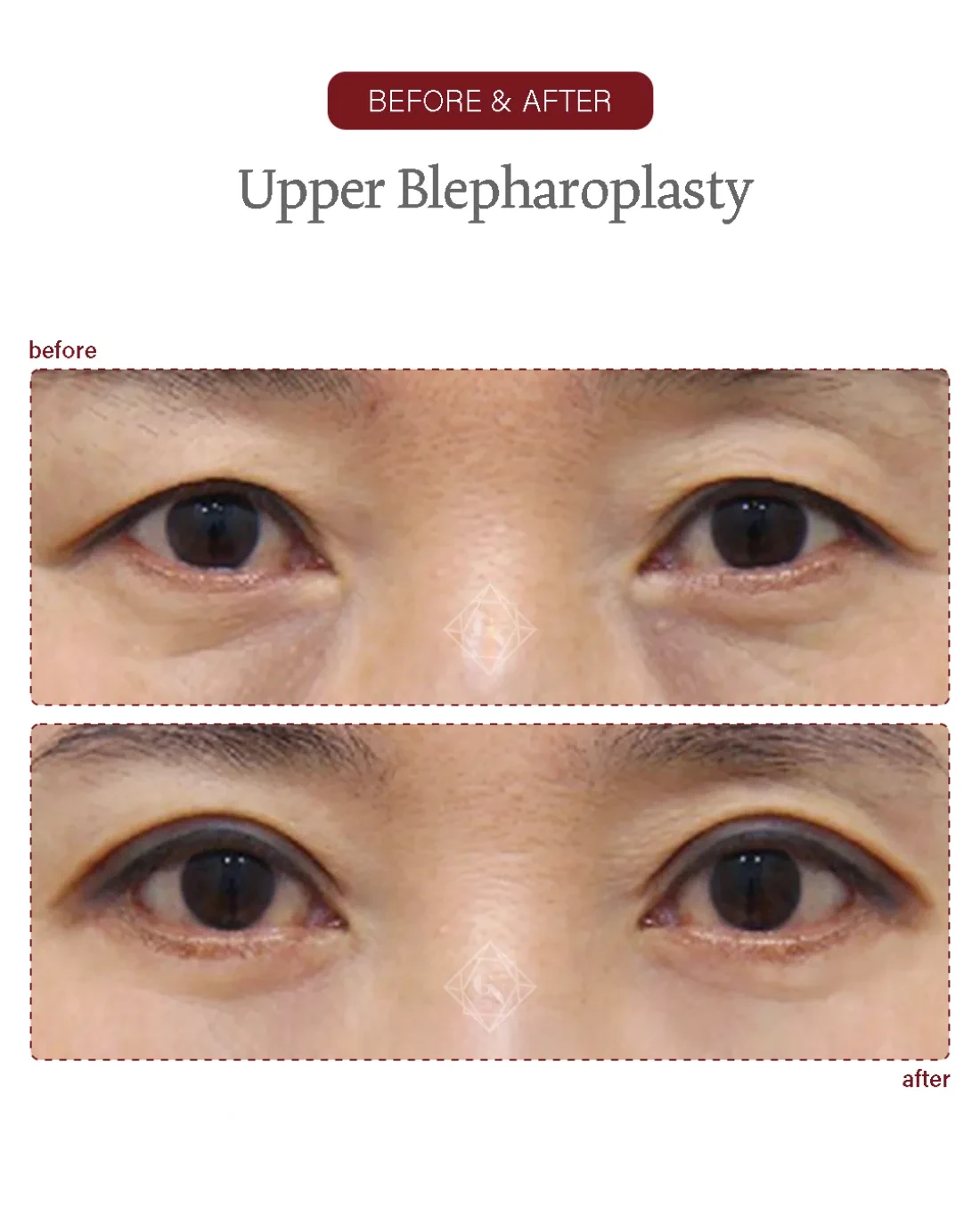
Eyelid before/after examples of actual Garnet patients (published with consent). Results, recovery and suitability vary by individual and are not guaranteed; the right approach is decided at an in-person consultation.
An upper blepharoplasty removes redundant skin (and tidies tissue) from the upper eyelid to lift hooding and open a tired, heavy eye. At Garnet it is planned and performed by one board-certified plastic surgeon, Dr. In-Soo Baek, from consultation through every follow-up.
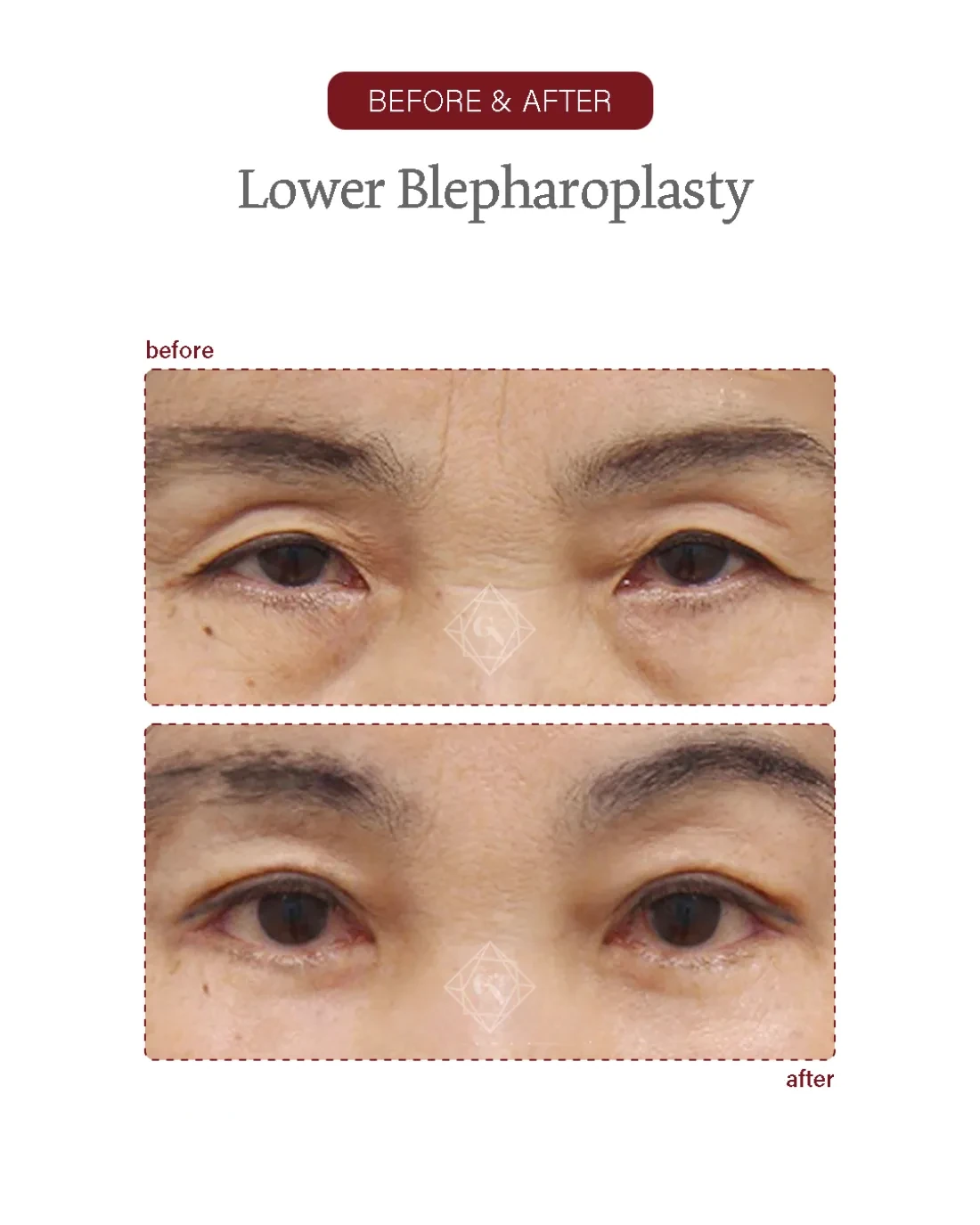
Eyelid before/after examples of actual Garnet patients (published with consent). Results, recovery and suitability vary by individual and are not guaranteed; the right approach is decided at an in-person consultation.

Garnet is well known for neck-wrinkle and lifting surgery. The facility is excellent and I’m thoroughly satisfied with the friendly consultation and the surgeon’s skill.
Director Baek In-soo, thank you so much. Thanks to you I keep getting told I look younger — it feels like I’ve gone back to my younger days.
I had upper and lower eyelid surgery and I’m really satisfied. The director and the manager were both so kind and clear.
I started with under-eye fat repositioning — the director and the manager are genuinely kind and good at what they do. I’ll be back.
I came on a referral and was very satisfied thanks to the doctor’s kind consultation and clear explanations. The nurses were friendly too.
I kept reading the reviews and came trusting the many mentions of skill and kindness. The clinic was busy with patients and spotless.
An upper blepharoplasty is an eyelid operation that removes the redundant fold of upper-lid skin (and tidies excess muscle or fat where present) through a fine incision hidden in the lid crease, so a heavy, hooded lid is lifted and the eye looks more open. It treats lax skin; where the lid itself sits low, it is paired with ptosis correction rather than replaced by it.
With age the upper-lid skin loosens and an overhanging fold develops — dermatochalasis — that can rest on the lashes, blunt the natural crease and make the eye look tired or, when heavy, narrow the field of vision. The cause is excess, lax skin (sometimes with a little bulging fat), so removing the redundant skin through a hidden crease incision lifts the hood and re-defines the fold.
Upper blepharoplasty treats the skin, not the height of the lid margin itself. If the eyelid margin sits low because the eye-opening (levator) muscle is weak — true ptosis — skin removal alone will not open the eye, and the two are planned together. Judging which problem is present, and how conservative to be with skin, is the heart of the consultation, particularly for an eyelid with a crease already present.
At Garnet this is a single-surgeon operation. Dr. Baek plans the case from the consultation, performs it himself and reviews healing at set intervals; the clinic caps the day at about two surgeries so each case has unhurried time. The stated aim is to address the concern you arrived with and to prevent foreseeable complications — particularly over-resection — rather than to chase the maximum possible change.
From the crease-line incision and conservative skin marking to closure — every step by Dr. Baek.

A single surgeon, start to finish. Dr. Baek plans the case, performs the operation himself and reviews every follow-up. The clinic caps the day at two surgeries, so each operation has unhurried time.
An upper blepharoplasty at Garnet typically runs about thirty to sixty minutes, usually under local anaesthesia with sedation as appropriate, decided with you after your medical history is reviewed. The steps below outline how it is carried out.
Dr. Baek assesses the lid in person — the amount of redundant skin, the crease, brow position and whether the lid margin sits low (ptosis) — and agrees the plan with you. The skin to remove is marked precisely, conservatively, with the eye open and closed.
A fine incision is placed in or just above the natural upper-lid crease, where the resulting scar settles into the fold and is hidden when the eye is open. The design is tailored to your existing crease and lid anatomy.
Only the marked redundant skin is removed; a strip of orbicularis muscle is tidied where it adds bulk. The aim is to lift the hood while leaving enough skin for the lid to close fully — over-resection is deliberately avoided.
Where a small pad of preaponeurotic fat bulges, it is conservatively reduced or repositioned to smooth the fold, rather than hollowing the lid.
The crease is re-formed at a natural height. Where the consultation shows it, ptosis correction or lower-lid surgery may be combined in the same sitting so the eyes match.
Fine closure with a light dressing. Because Garnet is single-surgeon, Dr. Baek reviews you himself before you settle in and at each follow-up; sutures come out at about seven days.
A few layers explain the hooded upper lid: the lid skin, which thins and stretches; the orbicularis oculi muscle beneath it; the orbital septum holding back small pads of preaponeurotic fat; and, deeper, the levator muscle and its aponeurosis, which open the eye and form the crease. Ageing dermatochalasis is mainly a skin-and-muscle problem, and conservative skin excision with the crease as the lower mark is the basis of a natural result (Aesthetic Plast Surg 2023; DOI 10.1007/s00266-023-03436-6).
Two cautions follow from the anatomy. First, removing too much skin can leave the lid unable to close fully or set the crease too high, so resection is measured and conservative — especially in a lid that already has a crease. Second, if the lid margin itself is low because the levator is weak, that is ptosis, a separate problem the skin operation will not fix; the consultation distinguishes the two so the right operation — or a combination — is planned. Where the heaviness comes mainly from a descended brow, a sub-brow lift may be more appropriate.
| Upper blepharoplasty | Sub-brow lift | Ptosis correction | |
|---|---|---|---|
| Problem treated | Excess upper-lid skin | Descended brow / outer hood | Low lid margin (weak levator) |
| What it does | Removes redundant lid skin | Lifts skin under the brow | Strengthens the eye-opening muscle |
| Scar | Hidden in the lid crease | Along the lower brow edge | Hidden in the lid crease |
| Opens the eye? | Lightens the hood | Lifts the brow-side hood | Yes — raises the lid margin |
| Typical candidate | Loose lid skin, normal lid height | Heavy outer brow, thick skin | Tired eye with low-sitting lid |
These often overlap and may be combined — the key is whether the heaviness comes from lid skin, the brow, or a low lid margin. Conservative skin excision underpins a natural upper-lid result (Aesthetic Plast Surg 2023; DOI 10.1007/s00266-023-03436-6). A descended brow may suit a sub-brow lift, and a low lid margin needs ptosis correction; Dr. Baek advises at consultation.
An upper blepharoplasty is usually performed under local anaesthesia, with light sedation if you prefer, decided with you for comfort over a thirty-to-sixty-minute operation. Your medical history and any dry-eye tendency are reviewed beforehand.
Because Garnet caps the day at about two surgeries, the operation is unhurried and the same surgeon who planned the case carries it out and reviews recovery — there is no separate operating doctor and no rotation of care.
Garnet is registered with Korea's foreign-patient programme; pre-operative checks, scheduling and after-care are coordinated for international visitors in English.
If the heaviness is really from the brow or a low lid margin, that is said at the consultation and the right operation planned. Photos can be reviewed before you travel.
An upper blepharoplasty incision is placed in or just above the natural upper-lid crease, so the resulting scar sits within the fold and is hidden when the eye is open. Closed with fine sutures and following the existing crease, it usually settles into a thin, inconspicuous line as it matures. Because the scar hides in the crease, upper-lid surgery generally leaves no visible mark in everyday settings.
Scars are permanent but designed to disappear into the crease; healing varies by individual and skin type, and an early pink line softens over the following months. Dr. Baek reviews scar maturation at the 1-, 3- and 6-month visits and advises on scar care; sun protection on the healing line is encouraged until cleared.
Keep the head elevated, use cold compresses early, take medication and any eye drops as prescribed, sleep on your back, and keep your follow-up visits.
Rubbing the eyes, strenuous exercise and heavy lifting early on, alcohol and smoking, very hot showers/saunas, eye make-up on the incision until cleared, and direct sun on the healing scar.
An upper blepharoplasty does not stop the lid ageing, but removing redundant skin gives a long-lasting result because the excess that caused the hood is gone. Published series and a systematic review report durable improvement with high patient satisfaction and few complications (Aesthetic Plast Surg 2023; DOI 10.1007/s00266-023-03436-6). Most patients do not need a repeat for many years.
Individual longevity depends on skin quality, sun exposure, weight change and how the brow and lid age afterwards. The skin slowly continues to relax over time, and a small amount of hooding can return years later. Garnet's approach is conservative skin removal so the lid still closes fully and the crease sits naturally, since an upper lid that was never over-resected ages more gracefully.
Where the lid margin sits low as well, ptosis correction opens the eye while the hood is lifted, so the result looks alert rather than merely de-bulked.
Many patients plan lower blepharoplasty in the same sitting, since the upper and lower lids age together and a balanced result looks more rested.
An incision or non-incision double-eyelid may be combined where crease definition is part of the wish.
Where the heaviness is mostly from the brow, a sub-brow lift can be planned instead of or alongside lid-skin removal for a balanced upper face.
Every operation carries risk. For upper blepharoplasty the main concerns are over-resection (too much skin removed, which can leave the lid unable to close fully and cause dryness) and asymmetry between the two creases; this is why the skin to remove is marked conservatively. Most reported complications in published series are minor and patient satisfaction is high (Aesthetic Plast Surg 2023; DOI 10.1007/s00266-023-03436-6).
Other possible risks include temporary swelling and bruising, dryness or watering, a crease set a little high or low, scar-related issues and, rarely, the need for a touch-up. Pre-existing dry eye can be aggravated and is assessed beforehand. These are explained individually at consultation.
What reduces risk in practice: distinguishing lax skin from true ptosis or a brow problem, conservative skin marking with the eye open and closed, fine closure in the crease, and follow-up by the operating surgeon. Garnet's single-surgeon, low-volume model is built around exactly this kind of unhurried planning and personal after-care. Results are intended improvements, not guarantees.
Most international patients plan roughly 7–10 days in Korea for an upper blepharoplasty, so sutures can be removed by the surgeon at about day seven and the early swelling has settled before travel. The coordinator confirms the timing for your specific plan.
Before you travel, send clear photos (eyes open, eyes gently closed, and a relaxed three-quarter view) and a note on your concern and dates through WhatsApp, LINE or the form below. You'll get an honest pre-assessment — including whether the issue is skin, brow or a low lid margin — rather than a hard sell.
Garnet is registered with Korea's foreign-patient programme and coordinates consultations, scheduling and after-care in English. After you return home, Dr. Baek can continue to review your recovery by messenger.
| Upper blepharoplasty | Sub-brow lift | Ptosis correction | |
|---|---|---|---|
| Problem treated | Excess upper-lid skin | Descended brow / outer hood | Low lid margin (weak levator) |
| What it does | Removes redundant lid skin | Lifts skin under the brow | Strengthens the eye-opening muscle |
| Scar | Hidden in the lid crease | Along the lower brow edge | Hidden in the lid crease |
| Opens the eye? | Lightens the hood | Lifts the brow-side hood | Yes — raises the lid margin |
| Typical candidate | Loose lid skin, normal lid height | Heavy outer brow, thick skin | Tired eye with low-sitting lid |
Citations are provided for general education. This page is informational and does not replace an in-person consultation; suitability, technique and recovery are individual.
Send photos and your question before you travel. An English-speaking coordinator reviews every enquiry and replies with honest guidance on whether surgery is appropriate, the likely plan and timing.
Prefer to chat now? Reach the coordinator directly: